
Why Babies Get Rashes While Taking Amoxicillin
Seeing a rash on your baby during a course of amoxicillin can be alarming. Many parents immediately worry: Is this a penicillin allergy? The reassuring truth is that a rash during amoxicillin treatment is fairly common in children, and many rashes are not true allergies. Some are caused by viruses, some are non-allergic drug reactions, and a smaller portion are immediate allergic reactions that require urgent care.
Amoxicillin (a penicillin-type antibiotic) is often prescribed for ear infections, pneumonia, sinus infections, and certain throat infections. Babies and young children frequently catch viruses around the same time they develop bacterial infections (or are mistakenly treated for one), which can make it tricky to figure out what’s causing the rash.
This article will help you understand common rash patterns, when to call your child’s clinician, which symptoms are emergency red flags, and how to handle future antibiotic decisions safely.
Amoxicillin Rash vs. True Allergy: What’s the Difference?
Parents often use the word “allergy” to mean any reaction. Medically, a true allergy involves the immune system reacting to the medication, sometimes in a rapid, dangerous way. A non-allergic rash may appear during treatment but does not necessarily mean your child must avoid penicillins forever.
Common types of rashes seen with amoxicillin
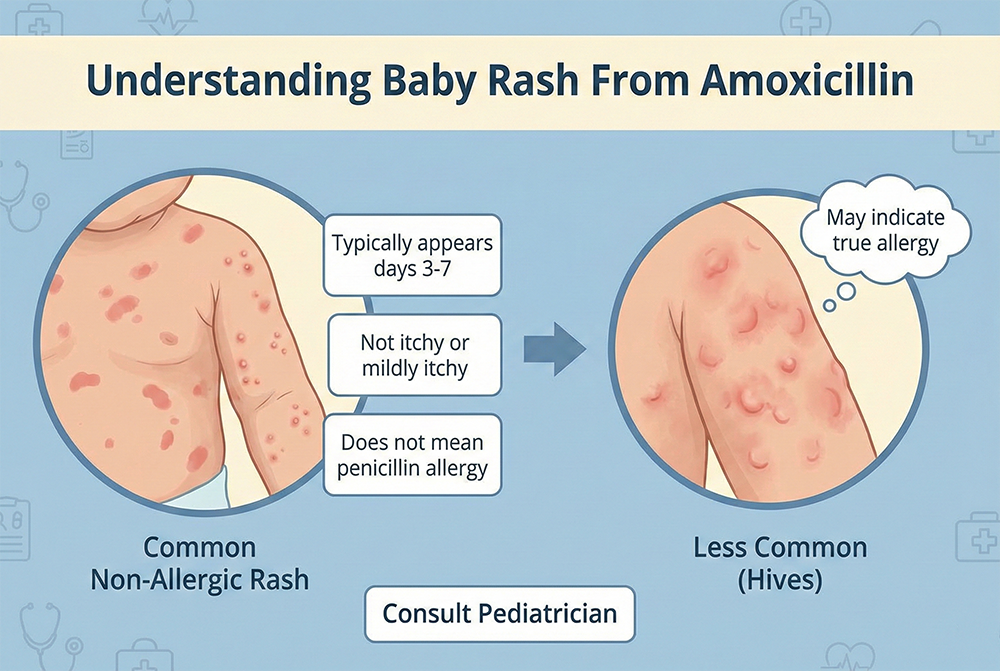
- Non-allergic “amoxicillin rash” (maculopapular rash): Flat and slightly raised pink or red spots/bumps, often starting on the trunk and spreading. Usually mild and not dangerous.
- Hives (urticaria): Raised, itchy welts that can move around the body and change shape/size. More suggestive of an allergic reaction, especially if it appears soon after a dose.
- Viral exanthem: A widespread rash caused by a virus. It can look similar to a non-allergic amoxicillin rash and may appear even without antibiotics.
- Contact/irritant rash: Localized redness where saliva, drool, wipes, or diaper friction irritates skin. Often unrelated to the medicine.
Timing matters
When the rash appears can give an important clue:
- Within minutes to 2 hours after a dose: More concerning for an immediate allergic reaction, especially if accompanied by hives, swelling, or breathing symptoms.
- After several days (often day 3–10): More typical of a delayed maculopapular rash or viral rash, which is often not a dangerous allergy.
What Does a Typical Non-Allergic Amoxicillin Rash Look Like?
A classic non-allergic amoxicillin rash (also called a delayed maculopapular eruption) often has these features:
- Appearance: Small pink-red spots or bumps, sometimes merging into larger patches.
- Location: Frequently begins on the chest, back, or belly and spreads to the face, arms, and legs.
- Itch: Often mild or not itchy (though some children do itch).
- Baby’s overall condition: Many babies otherwise seem okay—maybe still sick from the infection, but not suddenly worsening after each dose.
- Course: Can last several days and gradually fade.
Why it happens
In many cases, the rash happens because the immune system is activated by an underlying virus while the baby is taking the antibiotic. This is famously associated with infectious mononucleosis (Epstein–Barr virus) in older children, but younger children can also develop virus-related rashes during antibiotic treatment. Importantly, this kind of rash does not automatically mean your child has a lifelong penicillin allergy.
Signs the Rash May Be an Allergic Reaction
Some symptoms make an allergy more likely. Contact your child’s clinician promptly if you notice:
- Hives: Raised, itchy welts that come and go or move around.
- Swelling (angioedema): Puffy lips, eyelids, face, or tongue.
- Rash appearing quickly after a dose: Especially within 1–2 hours.
- Itching that is intense: More common with hives than with maculopapular rashes.
- Reactions that recur with each dose: A pattern of worsening soon after dosing can be important.
Emergency warning signs (call emergency services immediately)
Seek emergency care right away if your baby has any of the following:
- Trouble breathing, wheezing, noisy breathing, or repetitive coughing
- Hoarse voice or difficulty swallowing
- Sudden sleepiness or limpness
- Repeated vomiting with hives or swelling
- Widespread hives plus any breathing or circulation symptoms
- Signs of anaphylaxis (a severe allergic reaction)
Rare but Serious Reactions to Know About
Severe skin reactions to antibiotics are uncommon, but it helps to recognize red flags. If any of these occur, stop the medication unless a clinician advises otherwise and seek urgent medical evaluation.
Stevens-Johnson syndrome (SJS) / Toxic epidermal necrolysis (TEN)
- Clues: Painful rash, blistering, skin peeling, sores in the mouth/eyes/genitals, fever, and a very ill-appearing child.
DRESS syndrome (Drug Reaction with Eosinophilia and Systemic Symptoms)
- Clues: Rash plus fever, facial swelling, swollen lymph nodes, and signs of organ involvement (like unusual fatigue, jaundice, or dark urine). Typically occurs later rather than immediately.
Serum sickness–like reaction
- Clues: Hives or rash with joint pain/swelling and fever, often after several days of treatment.
What Should Parents Do If a Rash Appears?
Your next steps depend on how your baby looks overall and what the rash is doing. When in doubt, it’s appropriate to contact your child’s pediatric clinician the same day for guidance.
Step 1: Check for emergency symptoms
If there are any breathing issues, facial swelling, vomiting with hives, or your baby seems suddenly unwell, treat it as urgent.
Step 2: Document the rash
Before it changes, take a few clear photos in good lighting. Note:
- When the rash started
- Which day of antibiotics it is
- Time between the last dose and rash onset
- Whether it itches
- Any other symptoms (fever, diarrhea, swelling, cough)
Step 3: Don’t stop or continue blindly—get tailored advice
Whether to continue amoxicillin depends on the rash type, the infection being treated, and your baby’s symptoms. Some mild, delayed, non-itchy rashes may not require stopping, while hives or swelling typically prompt discontinuation and an alternative antibiotic.
Important: Do not give leftover antibiotics, and do not restart amoxicillin later without medical advice if an allergic reaction is suspected.
Step 4: Support comfort safely (with clinician guidance)
- Itch relief: Ask your clinician about an age-appropriate antihistamine if itching/hives are present.
- Skin care: Use lukewarm baths, fragrance-free moisturizers, and loose cotton clothing.
- Avoid new products: Skip new lotions, detergents, or topical treatments that could confuse the picture.
Could It Be a Viral Rash Instead of an Amoxicillin Allergy?
Yes. Viral rashes are extremely common in babies and toddlers and can show up during an illness for which amoxicillin was prescribed. Many viruses cause a widespread rash as the immune system responds. In these cases, the rash may appear even if the antibiotic played no role.
Clues that point toward a viral exanthem
- Other viral symptoms (runny nose, cough, watery eyes)
- Rash appears as fever is breaking
- Rash looks widespread but baby is otherwise stable
- No hives, no facial swelling, no breathing symptoms
Diaper Rash, Yeast Rash, and Amoxicillin: A Common Connection
Amoxicillin can change the balance of bacteria and yeast on the skin and in the gut. Some babies develop diaper rash during or after antibiotics, and some develop a yeast (candida) diaper rash.
How to tell a yeast diaper rash
- Bright red rash with sharp borders
- Small red “satellite” spots outside the main rash
- Involves skin folds (creases), where moisture sits
- May not improve with usual barrier cream alone
What helps
- Frequent diaper changes and gentle cleaning
- Air time (let the area breathe)
- Thick barrier ointment (zinc oxide or petrolatum)
- If yeast is suspected, your clinician may recommend an antifungal cream
Will My Baby Need to Avoid Penicillin Forever?
Not necessarily. Many children labeled “penicillin-allergic” are not truly allergic, especially when the only symptom was a delayed, non-hive rash during an illness. An inaccurate allergy label can matter because it may lead to broader-spectrum antibiotics that can be less ideal, cause more side effects, or contribute to antibiotic resistance.
How clinicians evaluate suspected amoxicillin allergy
Your child’s clinician may recommend:
- Detailed history: Timing, rash type, other symptoms, prior exposures.
- Allergy referral: Particularly if hives, swelling, or quick onset occurred.
- Testing or supervised challenge: In some situations, an allergist may use skin testing and/or a medically supervised oral amoxicillin challenge to confirm or rule out allergy.
What to record for future visits
Keep notes in your baby’s health records:
- Name of antibiotic (amoxicillin vs. amoxicillin-clavulanate)
- Dose and start date
- Exact time rash started
- Photos
- Other symptoms (hives, swelling, breathing changes)
- What happened after stopping or continuing
When to Call the Pediatrician (Same Day)
Contact your baby’s clinician the same day if:
- The rash is widespread or rapidly spreading
- The rash is itchy, looks like hives, or comes and goes
- There is facial swelling or swelling of lips/eyes
- Your baby has a new fever after improving
- Your baby seems unusually fussy, lethargic, or unwell
- There are sores in the mouth, red eyes, or blistering
- Your baby is under 3 months old with any significant new rash during illness
Practical Home Care Tips While You Wait for Advice
If your baby is stable and you’re waiting to speak to a clinician, these supportive steps can help:
- Keep skin cool and dry: Overheating can worsen itching and redness.
- Dress in soft layers: Loose cotton helps reduce friction.
- Use gentle products: Fragrance-free cleanser and moisturizer.
- Avoid scratching: Keep nails trimmed; consider mittens for young babies if needed.
- Hydration: Offer feeds as usual; illness and rashes can coincide with mild dehydration.
What About Switching Antibiotics?
If a true allergy is suspected, clinicians may switch to a different antibiotic class. If the rash seems non-allergic, your clinician may recommend completing the course, depending on the infection and your child’s overall status.
Decisions about switching should weigh:
- The likelihood of allergy vs. viral rash
- How severe the infection is
- Whether symptoms are improving on amoxicillin
- Your baby’s age and medical history
How to Prevent Future Problems
While you can’t always prevent rashes, you can reduce risk and confusion in the future.
Use antibiotics only when truly needed
Antibiotics do not treat viruses. If your baby is prescribed amoxicillin, it’s okay to ask:
- What infection are we treating?
- Is this likely bacterial?
- Are there watch-and-wait options (for example, in some ear infections)?
- What signs mean we should recheck?
Give medication exactly as directed
- Use the provided syringe for accurate dosing
- Do not skip doses or double up without instructions
- Store as directed (some suspensions require refrigeration)
Clarify the “allergy” label
If your child had a rash, ask whether it should be documented as a side effect, non-allergic rash, or suspected allergy. Precise documentation helps future clinicians make safer choices.
A Reassuring Bottom Line
A baby rash from amoxicillin can be scary, but it is not always an allergy. Hives, swelling, breathing symptoms, or rapid onset after a dose are more concerning and need prompt evaluation. A delayed, spotty rash without other alarm symptoms is often non-allergic or virus-related, but it still deserves a call to your child’s clinician for individualized guidance.
You’re not overreacting by checking—your careful attention is exactly what keeps your baby safe. With good documentation and, when appropriate, allergy evaluation, many children can avoid being incorrectly labeled penicillin-allergic and can receive the best antibiotic choices in the future.


